Endurance | Mobility | News/Media | Strength | Tidbits
Why The “Strengthification” Of Gen X’ers & Baby Boomers Is The Greatest Health Challenge Of The 21st Century
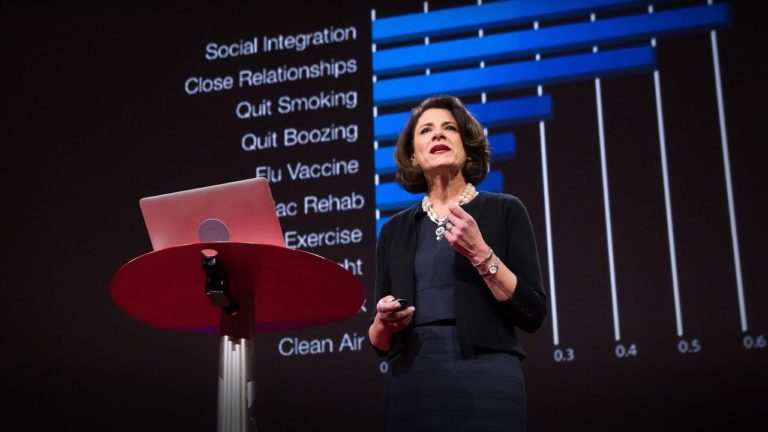
Last October l presented at the Ancestral Health Society of New Zealand (AHSNZ) International symposium with the title of my talk: “Why the “strengthification” of Gen X’ers & Baby Boomers is the greatest health challenge of the 21st century”. In this session I discussed a number of things in relation to ageing and the dynapenic/sarcopenic…