

Creatine and Resistance Training in Older Adults: What the Evidence Really Shows (Updated 2026)
What is Creatine?
The use of creatine (Cr) can be traced back to the early 1990s when several elite sprint athletes reported performance-enhancing benefits following gold medal winning performances at the 1992 Barcelona Olympic Games (Anderson, 1993). This sparked the birth of a new era with creatine gaining widespread popularity as a legitimate ergogenic aid (Bird, 2003). Creatine is a nitrogenous organic acid abundant in metabolically active muscle, heart and brain tissue. It is synthesised endogenously in the liver and kidneys from the amino acids arginine, glycine and methionine, and absorbed from the diet primarily from red and white meat (Chilibeck et al., 2017; Phillips, 2015). Most creatine is stored intramuscularly as phosphocreatine (PCr) (Candow et al., 2014). PCr functions principally as a temporal energy buffer by donating a high-energy phosphate to ADP through the enzymatic reaction of creatine kinase, which re-synthesises and replenishes ATP stores and thus helps maintain skeletal muscle energy availability during very short, intense anaerobic exercise (Kreider et al.,, 2017; Candow et al., 2014; Candow & Chillibeck, 2010). PCr also acts as a spatial energy buffer shuttling intracellular energy between mitochondria and sites of cellular ATP utilization (Kreider et al., 2017; Gualano et al., 2016).


Creatine supplementation increases the Cr/PCr reservoir by 20-40% (Kreider et al., 2017) and it is posited that this enhances PCr-mediated ATP resynthesis during and after high-intensity exercise bouts (Deane et al., 2017; Close et al., 2016), thereby allowing greater amounts of work to be accomplished (Phillips, 2015). This is particularly relevant for resistance training1 given that a dose-response relationship has been shown to exist between training volume and gains in skeletal muscle mass (Schoenfeld et al., 2017a; Schoenfeld et al., 2017b), and muscle strength (Figueiredo et al., 2017; Ralston et al., 2017). Other possible mechanisms to account for creatine ergogenicity are reduced exercise-induced muscle damage, reduced oxidative stress, increased GLUT4 in muscle fibre membranes, increased cell swelling that activates protein synthesis within muscle fibres, and decreased reliance on anaerobic glycolysis/reduced lactate production (Chilibeck et al., 2017; Kreider et al., 2017; Devries and Phillips, 2014). Although the exact mechanisms of action are still to be determined (Phillips, 2015), creatine supplemented resistance training has been extensively researched, especially in younger populations (Buford et al., 2007; Kreider et al., 2017). Consuming 5 grams of creatine (or 0.3 grams per kilogram body weight) four times daily for 5-7 days is generally viewed as the most effective way to increase muscle creatine stores and can be adequately maintained by consuming 3-5 grams/day following this loading phase (Kreider et al., 2017).
Is Creatine Effective in Older Adults?
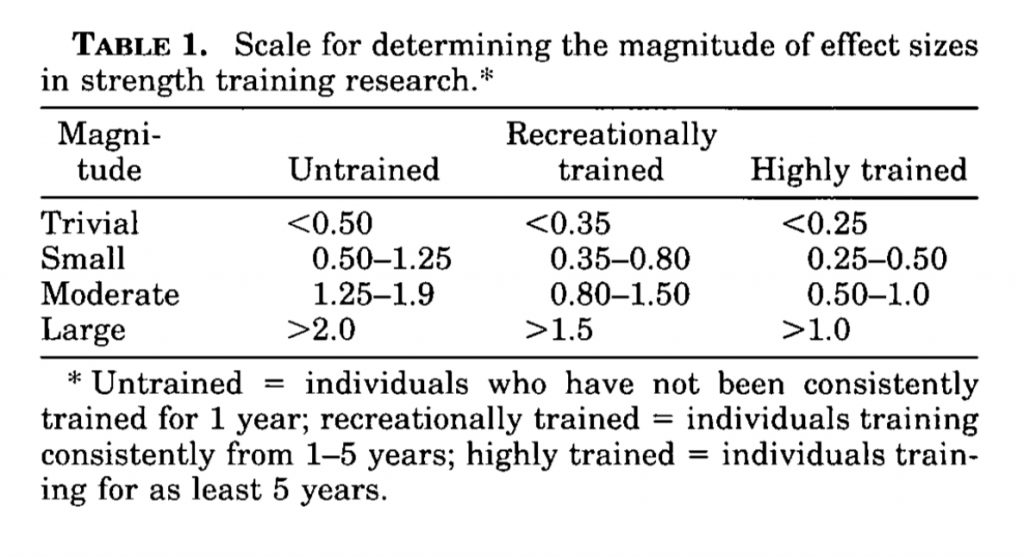
Over the past three decades, our understanding of age-related changes in skeletal muscle structure and function—and the role of resistance training in attenuating these changes—has evolved substantially. During this time, several systematic reviews and meta-analyses of randomised, placebo-controlled trials have examined the effects of creatine and resistance training in older adults on lean tissue mass and muscle strength in middle-aged and older adults (approximately 45–80 years) (Candow et al., 2014; Devries & Phillips, 2014; Chilibeck et al., 2017). Notably, Chilibeck et al. (2017; p.219) found that found significantly greater increases in lean tissue mass (1.4 kg; SMD=1.35), upper (i.e. chest press; SMD=0.37) and lower (i.e. leg press; SMD=0.25) body muscle strength when middle-aged to older adults (50-80 years old) were supplemented with creatine during resistance training. However, while the results of this study are often promoted as evidence that creatine has ergogenic value for this cohort, the standardised mean differences reported for muscle strength were trivial based on the effect sizes proposed by Rhea (2004) to delineate what is, and what is not meaningful following resistance training (see Table 1 below). If we apply more traditional effect sizes (Sullivan and Feinn, 2012), these strength improvements still remain small.
One of the longest trials to investigate the impact of creatine supplementation and resistance training in middle-aged and older male adults (49-69 years old) found no additional benefits on measures of bone, muscle or strength after 12 months (Candow et al., 2020). Moreover, Beaudart et al., (2018) concluded that the research findings are equivocal for creatine after conducting a systematic review into the effects of various nutrients on muscle mass, muscle strength and physical performance in older adults (≥60 years old).
More recently published meta-analyses and systematic reviews (Sharifian et al., 2025, Liu et al. 2025 and Davies et al. 2024) concur with those cited above. All consistently demonstrate that creatine supplementation, when combined with exercise and/or resistance training, results in significantly greater improvements in muscle strength and muscle mass in older adults and adults with chronic disease compared with placebo. However, across all these reviews the populations studied were typically defined as “older” using lower age thresholds (Sharifian uses ≥55 years and Liu uses ≥50), with most analyses pooling data from cohorts spanning middle age through to older adulthood. While these findings provide robust evidence that creatine can augment strength and muscle mass adaptations in aging populations broadly (40-80 years), they largely reflect heterogeneous samples that include substantial numbers of middle-aged adults rather than cohorts exclusively representative of later life. Worryingly, the systematic review by Liu et al. (2025) appears to have failed to include several studies that, by all accounts, meets their pre-defined study inclusion criteria which thereby raises questions regarding their findings and conclusions.
Surprisingly, and disappointingly, no meta-analysis has yet assessed the effects of creatine supplementation on resistance training outcomes – including lean skeletal muscle mass or lean body mass, muscle strength, muscle power and physical functionality – in adults exclusively 60 years or older. This is important because it cannot be assumed that middle-aged adults (40-60 years) and older adults (≥60 years) respond similarly to creatine supplemented training due to the significant and progressive physiological changes associated with aging. These include reductions in training tolerance, altered neuromuscular responsiveness, and longer recovery timelines, all of which may influence both the magnitude and time course of adaptation to resistance training.
Despite all the research that has been carried out thus far, the question as to whether creatine consistently augments or improves adaptations to resistance training in older adults (≥60 years old) remains largely unknown. Because of this, what I will now do is assess the body of evidence as it relates to older adults and let you be the judge. The key features of these studies are:
- Includes only older adults (≥60 years old)
- Performed resistance training
- Supplemented with creatine (monotherapy) vs placebo
- Included outcomes for –
- Muscle strength (or power if tested)
- Muscle mass (skeletal muscle or lean body mass)
- Physical function (e.g., 5TSTS, TUG, gait speed etc)
Published Studies in Older Adults (≥60 years)
At the time of writing these are the studies that have assessed the monotherapy supplementation of creatine versus placebo in older adults (≥60 years) undergoing resistance or exercise training (Amiri et al. 2023; Chilibeck et al. 2023; Roschel et al. 2021; Smolarek et al., 2020; Oliveira et al. 2020; Pinto et al 2016; Gualano et al., 2014; Aguiar et al., 2013; Alves et al., 2013; Candow et al. 2008; Deacon et al., 2008; Hass et al., 2007; Faager et al. 2006; Chilibeck et al. 2005; Brose et al 2003; Chrusch et al., 2001; Bermon et al., 1998)2.
Strength, Muscle Mass and Physical Function
Of those that measured changes in lean tissue (skeletal muscle) mass, participants supplemented with creatine consistently achieved greater benefits compared to placebo in 7 of 10 studies (70%) (Chilibeck et al. 2023; Gualano et al., 2014; Pinto et al 2016; Aguiar et al., 2013; Candow et al. 2008; Brose et al 2003; Chrusch et al., 2001). In contrast, the effects of creatine on muscle strength were less consistent with the majority of studies showing no additional benefit versus placebo for core compound lower limb exercises (i.e. leg press) in 9 of 15 studies (60%) (Chilibeck et al. 2023; Roschel et al. 2021; Pinto et al 2016; Gualano et al., 2014; Alves et al., 2013; Deacon et al., 2008; Faager et al. 2006; Brose et al 2003; Bermon et al., 1998). Six of the nine studies (66%) that explored the impact of creatine on physical function found no evidence of performance enhancement compared to placebo for a number of standard tests (Chilibeck et al. 2023; Roschel et al. 2021; Gualano et al. 2014; Aguiar et al., 2013; Gualano et al. 2011; Deacon et al., 2008; Hass et al., 2007; Faager et al. 2006; Brose et al 2003); examples of physical function tests included the 30-second chair stand test, 30 metre walk time, time to climb 14 stairs, the timed-up-and-go test, the shuttle walk distance test.
Dynamic Balance
So far, no randomised controlled trials have yet tested whether creatine supplementation in older adults (≥60 years) when used in conjunction with resistance or exercise training positively impacts balance. In older middle-aged adults, creatine was found to actually inhibit improvements in balance performance (Johannsmeyer et al., 2016). Those that were randomly allocated to the placebo group during drop-set resistance training achieved significantly greater improvements in dynamic balance (30.8%) compared to the creatine group (19.4%), with a reduction in balance errors detected for the placebo group only.
This raises an important and still unresolved question: in some situations, could adding creatine to resistance training support gains in muscle mass and strength in (some) older adults, yet fail to translate into improvements in balance? That question is especially relevant and future research needs to urgently establish if there is a trade off. Dynamic balance is critical in older adults for maintaining independence and mobility, and for reducing the risk of falls. In later life, falls are rarely trivial events. Beyond injury and hospitalisation, a fall—particularly one resulting in fracture—is associated with a significant increase in 1-year mortality, as well as accelerated functional decline and loss of independence. For many older adults, a single fall can mark the beginning of a downward spiral that is difficult to reverse.
It would also be remiss of me not to also mention that balance is also very skill-specific—that is, to optimally improve balance, you need to train balance—so research would need to explore the effect of creatine supplementation in older adults when combined with resistance training and/or balance exercise/training. Recently, a pilot study by Teixeira et al. (2024) interestingly found that creatine supplementation (without any exercise intervention) improved balance performance in sedentary non-sarcopenic older women.
Quality of Life
In relation to quality of life, there is virtually no research that has investigated whether creatine when supplemented with resistance training results in better outcomes. Amiri et al. (2023) found that while significant improvements were found for quality of life in older adults doing resistance training versus the control group (i.e. no resistance training), creatine supplementation with resistance training did not augment such QoL enhancements. Encouragingly, Neves et al., (2011) demonstrated improved quality of life and physical function in postmenopausal women (mean age=58 years old) with knee osteoarthritis that took creatine during resistance training.
Anomalous Data
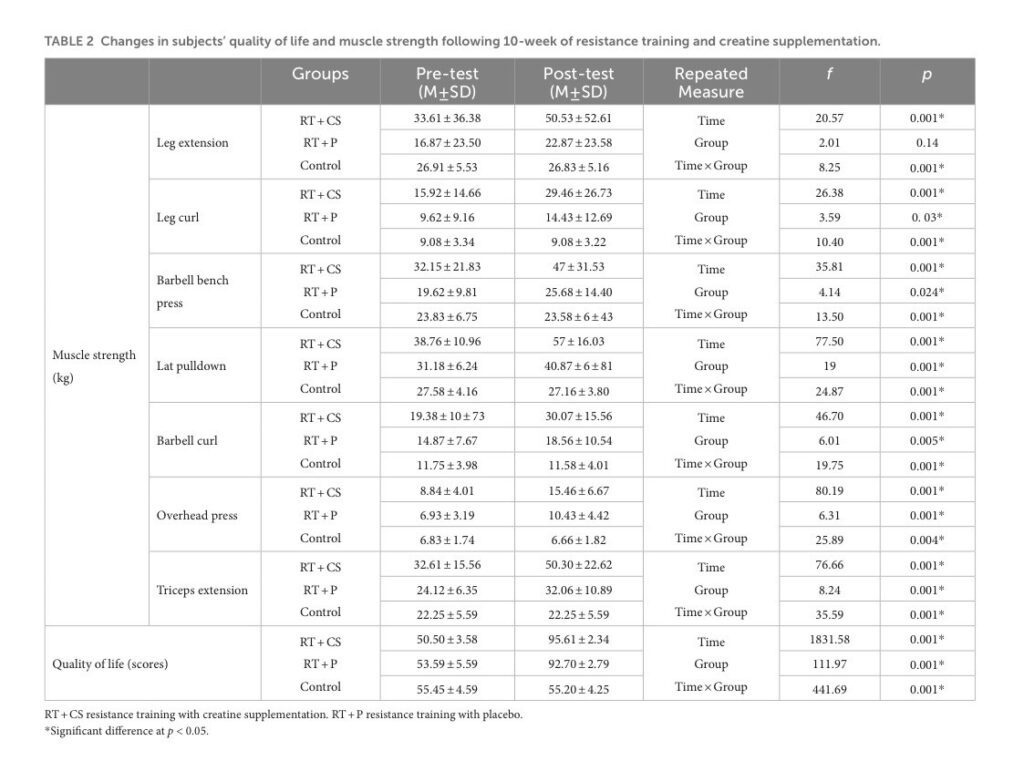
I wanted to point out that even in studies that did find greater gains in muscle strength in older adults supplemented with creatine, upon closer analysis some results are, and I can’t find a better way of putting this, just a bit weird. For example, Amiri et al. (2023) found that creatine supplementation in older adults substantially increased strength gains following resistance training (almost doubled for the leg extension exercise) compared to those in the placebo group. However, if you take a closer look at table 2 below from the study, there are huge differences in baseline strength levels. Now the authors report that no statistically significant differences at baseline were found, but the fact that the resistance training group supplemented with creatine were so much stronger is unusual given that the groups were supposedly randomly allocated. If we compare baseline differences for the leg extension exercise, the creatine-supplemented resistance training group was almost 100% stronger (33.6 vs 16.9). These results make me question whether the strength gains made during the study were confounded by comparing a ‘naturally’ stronger group of older adults, and perhaps more responsive to resistance training, than a much weaker placebo supplemented group. It is also possible that—even if randomly allocated—such strength differences at baseline occurred by chance. Insufficient power to detect real differences between groups is another possibility given groups only had 15 participants each, so while the authors claim that there were no statistically significant differences at baseline (p>0.05), in actuality there may have been.
Taken together, creatine supplementation in older adults during resistance training appears to support significantly greater increases in lean tissue or skeletal muscle mass compared to those not supplemented with creatine. Nonetheless, this has not necessarily translated consistently into appreciable improvements in multijoint lower limb muscle strength, physical function, balance and/or quality of life.
Is Creatine Well Tolerated and Safe?
Creatine when used in healthy, older adults appears to be well tolerated and safe. There have been no reports or evidence of any adverse effects that are serious in nature (Chilibeck et al., 2017; Goudarzian et al., 2017; Pinto et al., 2016; Gualano et al., 2014; Alves et al., 2013; Brose et al 2003; Chrusch et al., 2001; Bermon et al., 1998) and self-reported issues associated with the use of creatine have been uncommon (Pinto et al 2016; Gualano et al., 2014; Alves et al., 2013; Brose et al., 2003). No adverse events related to, nor changes in either kidney or liver function have been reported from RCTs (Gualano et al., 2014; Tarnopolsky et al., 2007; Brose et al., 2003) and other studies that included both middle-aged and older adults are devoid of any such side-effects (Johannsmeyer et al., 2016; Chilibeck et al., 2015; Lobo et al., 2015; Cornelissen et al., 2010; Eijnde et al., 2003). Some studies have reported that gastrointestinal (GI) distress and muscle cramping and/or muscle strain may be more common in those receiving creatine (Chilibeck et al., 2015; Chrusch et al., 2001). In healthy, older men (mean age=70 years old) loose stools were reported by Chrusch et al., (2001) as a side-effect during the 1-week loading phase and increased muscle cramping/strain occurred between weeks 3 and 5. Middle-aged to older postmenopausal women (mean age=57 years old) taking creatine experienced a higher number of these adverse events when GI complaints and muscle cramping were grouped for assessment (Chilibeck et al., 2015). None of these side-effects led to study discontinuation and appear to be transient in nature with no impairment of exercise training response noted.
The following tables outline adverse events recorded over long-term trials.
Adverse Events – Creatine vs Placebo (1-year trial)
| Category | Finding | Creatine Group | Placebo Group |
|---|---|---|---|
| Total supplement-related adverse events | All events classified as mild | 5 participants | 2 participants |
| Gastrointestinal issues | Indigestion, diarrhoea, bloating | 5 participants | 2 participants |
| Muscle cramping | Self-reported cramps | 2 participants | 2 participants |
| Resistance Training-Related Adverse Events (Both Groups) | |||
| Total training-related events | Muscle soreness and joint pain | 54 total events | |
| Causality | 43 possibly caused • 7 probably caused • 4 definitely caused | ||
| Severity | 50 mild • 4 moderate | ||
| Biochemistry – Creatine Group | |||
| Liver enzymes | AST & ALP elevated at various timepoints | 2 participants with elevated AST; 1 also with elevated ALP | |
| Urine creatinine | Elevated at various timepoints | 13 participants (5 with high serum creatinine also) | |
| Biochemistry – Placebo Group | |||
| Bilirubin | Elevated at 12 months | 1 participant | |
| Renal markers | Low urine creatinine & creatinine clearance (12 months) High creatinine (various times) |
1 low clearance participant 11 high creatinine (1 also high serum creatinine) |
|
All supplement-related adverse events were mild. The majority of adverse events were associated with the resistance-training program and were also predominantly mild.
Adverse Events – Creatine vs Placebo (2-year trial)
| Adverse event (kidney) | Creatine group participants / events / counts |
Placebo group participants / events / counts |
Notes on severity & relationship |
|---|---|---|---|
| Total kidney-related events | 15 participants / 20 events | 21 participants / 24 events | All kidney AEs were rated “possibly related” and mostly mild, except one moderate kidney infection (creatine). |
| High urine albumin–creatinine ratio (ACR) | 2 participants | — | Mild; possibly related. |
| High urine microalbumin | 3 participants | 6 participants | Mild; possibly related. |
| Hemoglobin in urine (hematuria) | 3 participants | 8 participants | Mild; possibly related. |
| Low creatinine clearance | 1 participant | 2 participants | Mild; possibly related. |
| High blood creatinine | 6 participants | — | Mild; possibly related. |
| Low estimated glomerular filtration rate (eGFR) | 4 participants | — | Mild; possibly related. |
| Protein in urine (proteinuria) | — | 6 participants | Mild; possibly related. |
| Low urine creatinine | — | 1 participant | Mild; possibly related. |
| Kidney cysts | — | 1 participant | Mild; possibly related. |
| Kidney infection | 1 participant | — | Moderate severity (creatine). Rated possibly related. |
| Adverse event (liver) | Creatine group | Placebo group | Notes on severity & relationship |
|---|---|---|---|
| Total liver-related events | 9 events in 7 participants | 6 events in 5 participants | All liver AEs were rated “possibly related” and mild. |
| Elevated liver enzymes (AST / ALT) | 6 participants | 3 participants | Mild; possibly related. |
| Bilirubin in urine | 1 participant | — | Mild; possibly related. |
| Low albumin | 1 participant | 2 participants | Mild; possibly related. |
| Adverse event (GI) | Creatine group | Placebo group | Severity & relationship notes |
|---|---|---|---|
| Total GI events | 13 events in 13 participants | 17 events in 14 participants | Classified as possibly/probably/definitely related. Mostly mild, but with some moderate and one severe event (see rows below). |
| Bloating / acid reflux / heartburn | Heartburn: 1 (moderate reported) | Heartburn: (moderate reported in overall text; group not consistently specified) | Heartburn instances included at least one moderate case (creatine and/or placebo reported in source text). |
| Constipation | — | Constipation: 1 (moderate reported) | One moderate constipation case reported (group attribution in source text ambiguous). |
| Diarrhea | — | 2 cases (moderate) | Two moderate diarrhea cases reported in the placebo group. |
| Nausea | — | 2 cases (one moderate, one severe) | Both nausea events reported in the placebo group (one moderate, one severe). |
| Upset stomach | 1 case (moderate) | — | Moderate upset stomach reported in the creatine group. |
| Other GI (bloating, reflux) | Included among 13 events | Included among 17 events | Mostly mild and possibly/probably/definitely related. |
| Description | Creatine | Placebo | Severity & relationship |
|---|---|---|---|
| Reported muscle cramps | 2 participants | 2 participants | Two events rated mild and two moderate in total (one moderate in each group). Rated possibly/probably related. |
| Description | Details | Severity & relationship | |
|---|---|---|---|
| Total other musculoskeletal events | n = 172 events (related to exercise training) | Mostly mild or moderate; rated possibly/probably/definitely related to intervention (exercise). | |
| Typical events | Muscle soreness, joint pain, tendonitis, pain in Achilles/plantar/anterior tibia | One case rated severe (tendonitis & multi-site pain: Achilles, plantar fascia, anterior tibia). | |
| Drops / accidental injuries | One participant dropped a 5-lb weight on toe → bruising | Mild bruising reported. | |
| Falls during walking intervention (4 participants) |
– Swollen knee (moderate) – Neck & upper back pain (moderate) – Tailbone pain (moderate) – Shoulder pain (mild) |
These were classed as intervention-related injuries from falls during walking/treadmill activity. | |
| Outcome | Creatine group | Placebo group | Notes |
|---|---|---|---|
| Serious intervention-related adverse events | 0 | 1 (fall off treadmill → swollen knee) | Only one AE was rated “serious” (placebo group) because it caused impairment to everyday activities. |
| Withdrawals due to adverse events | 2 withdrawals (diarrhea; self-reported metal allergy to equipment) |
1 withdrawal (injury after treadmill fall) |
Three participants withdrew in total: two creatine, one placebo. |
Summary: Adverse events were similar between creatine and placebo groups and were predominantly mild. Kidney and liver events were labelled “possibly related” to the intervention; only one intervention-related serious event occurred (placebo group).
What Questions Remain Unresolved?
Many questions remain unresolved. Despite the evidence supporting increased lean tissue mass following creatine supplementation, it seems too early to claim definitively that such a strategy substantially and consistently improves muscle strength or physical function in all older adults undergoing resistance training. Training adaptations, in theory, should be augmented by creatine. It is well acknowledged that aging causes skeletal muscle atrophy with disproportionately greater reduction in cross-sectional area (CSA) of PCr-rich type-II muscle fibres (Nilwik et al., 2013; Kushmerick et al., 1992), and this results in much lower levels of intramuscular creatine in the quadriceps vastus lateralis (thigh) muscle of older versus younger adults (Chilibeck et al., 2017). Lifestyle changes with aging – particularly reduced dietary meat intakes, decreased physical activity levels (Chilibeck et al., 2017) and increased sedentary time (Diaz et al., 2017; Dunlop et al., 2015) – may further impact muscle PCr levels and modify any potential benefits of creatine supplementation. Further research is therefore required to establish whether the magnitude and heterogeneity of resistance training adaptations is modulated by significant inter-individual differences in creatine uptake kinetics, given that training responsiveness is correlated to the change in intramuscular creatine stores.
Why Older Adults May Respond Differently to Creatine
Research by Syrotuik and Bell (2004) provide support for this possibility where it was demonstrated that young, healthy men had 3 different levels of response to a 5-day creatine load as measured by post-supplementation intramuscular creatine levels (see figure 2 below). Responders to creatine loading possessed a biological profile of the lowest initial muscle Cr/PCr levels, greatest percentage of type-II muscle fibres, largest muscle fibre CSA and lean tissue mass, plus were the only subjects to achieve improvement in 1RM leg press when compared to quasi- and non-responders. It is plausible that this may partially account for the lack of consistency in the research as such inter-individual variation could significantly water down any generalised group benefits.
This research also raises another potential limitation in those older adults that are most in need of an ergogenic effect—that is, those with sarcopenia, muscle weakness and fragilty—as they may be the least likely, when assessed against these bioloigical responder profiles, to reap the meaningful benefits of creatine supplementation. Furthermore, it is well accepted that intramuscular post-supplementation creatine levels (at day 28) are comparable for “slow” (3 grams/day for 1 month) and “rapid” load (4×5 grams/day for 5-7 days and 3-5 grams/day thereafter) protocols (Hultman et al., 1996). Thus, it would be prudent to compare whether the slow load approach is better tolerated than the rapid load approach (i.e. reduction of GI-related side-effects and muscle cramping/pulls) based on the evidence where some older adults appear to be more sensitive to large initiation doses of creatine.

Potential Other Benefits of Creatine in Older Adults
While creatine is best known for improving muscle mass and strength when combined with resistance training, research in older adults suggests several additional potential benefits relevant for healthy aging.
Cognitive Function & Brain Energy
Creatine plays a key role in brain energy metabolism. Randomised trials and meta-analyses suggest small but consistent improvements in memory and information processing, particularly in older adults or during cognitively demanding conditions. Effects appear more pronounced when brain energy availability is compromised. The meta-analysis by Prokopidis and colleagues (2023) showed improved memory performance, with larger effects observed in older adults compared to younger cohorts.
Cognitive Performance During Sleep Deprivation
One of the clearest non-muscle effects of creatine is its ability to attenuate cognitive decline during sleep deprivation. Controlled studies show better reaction time, working memory and reduced mental fatigue following acute or short-term creatine supplementation. Creatine reduced cognitive performance decline after sleep deprivation compared with placebo (Gordji-Nejad et al. 2024).
Mood & Depressive Symptoms
Creatine has been studied as an adjunct treatment for depression, likely via effects on brain bioenergetics and neuroplasticity. A recent meta-analysis reports a small reduction in depressive symptoms, though overall evidence quality is low and effects are modest. Pooled effect size ≈ −0.34 SMD vs placebo; below minimal clinically important difference (Eckert et al. 2025).
Vascular Endothelial Function
Pilot research demonstrated that creatine supplementation without any exercise intervention improved several indices of vascular endothelial function in 50-64 year old men and women (Clarke et al. 2025).
Metabolic Health (Triglycerides & Glucose)
Limited evidence in older adults suggests creatine may modestly reduce fasting triglycerides and glucose, though findings are based on small trials and are not yet consistent enough to support clinical recommendations.
Bone Health
Creatine has been investigated as a potential adjunct to resistance training for bone health. While some individual studies report favourable changes in bone turnover markers, meta-analyses show no consistent improvement in bone mineral density (Sharifian et al. 2025).
Practical Take-Home Message
So let’s bring this all together.
Based on the available short and long-term studies in older adults, creatine supplementation appears to be safe to consume and offers some healthy-aging benefits. Evidence is strongest for increased skeletal muscle mass when compared to placebo. However, research does not consistently demonstrate additional improvements in muscle strength for compound lower-limb exercises such as the leg press, nor—perhaps most importantly—physical function in the majority of studies. My professional opinion is that the effect size—that is, how beneficial creatine supplementation is compared to no supplmentation—varies within older adults largely due to differences in individual creatine responder profiles. Muscle creatine uptake varies substantially between individuals, which in turn modulates the training stimulus, its effectiveness, and eventual outcomes. Beyond skeletal muscle mass and strength, creatine may support brain energy availability, cognitive performance under sleep deprivation, and possibly mood. However, effects on metabolic health are less consistent, and for bone density and balance, current data suggests that creatine does not confer additional benefits beyond those achieved with exercise alone.
AUTHOR: Sean Wilson
PUBLISHED: January 2026
The original 2021 article, “Is Creatine As Good As It’s Cracked Up To Be? Older Adults and Resistance Training” is available for those interested in reviewing how things have changed over the last few years.
References
Aguiar AF, Januário RS, Junior RP, Gerage AM, Pina FL, Do Nascimento MA, Padovani CR, Cyrino ES. Long-term creatine supplementation improves muscular performance during resistance training in older women. European journal of applied physiology. 2013 Apr 1;113(4):987-96.
Alves CR, Merege Filho CA, Benatti FB, Brucki S, Pereira RM, de Sá Pinto AL, Lima FR, Roschel H, Gualano B. Creatine supplementation associated or not with strength training upon emotional and cognitive measures in older women: a randomized double-blind study. PLoS One. 2013 Oct 3;8(10):e76301.
Amiri, E., & Sheikholeslami-Vatani, D. (2023). The role of resistance training and creatine supplementation on oxidative stress, antioxidant defense, muscle strength, and quality of life in older adults. Frontiers in public health, 11, 1062832.
Anderson O. (1993) Creatine propels British athletes to Olympic gold medals: Is creatine the one true ergogenic aid? Running Research News 9, 1-5
Beaudart C, Rabenda V, Simmons M, Geerinck A, Araujo DC, Reginster JY, Amuthavalli TJ, Bruyère O. Effects of Protein, Essential Amino Acids, B-Hydroxy B-Methylbutyrate, Creatine, Dehydroepiandrosterone and Fatty Acid Supplementation on Muscle Mass, Muscle Strength and Physical Performance in Older People Aged 60 Years and Over. A Systematic Review on the Literature. The journal of nutrition, health & aging. 2018;22(1):117.
Bermon S, Venembre P, Sachet C, Valour S, Dolisi C. Effects of creatine monohydrate ingestion in sedentary and weight-trained older adults. Acta Physiologica Scandinavica. 1998 Oct 1;164:147-56.
Bird SP. Creatine Supplementation and Exercise Performance: A Brief Review. Journal of Sports Science & Medicine. 2003;2(4):123-132.
Brose A, Parise G, Tarnopolsky MA. Creatine supplementation enhances isometric strength and body composition improvements following strength exercise training in older adults. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 2003 Jan 1;58(1):B11-9.
Buford TW, Kreider RB, Stout JR, Greenwood M, Campbell B, Spano M, Ziegenfuss T, Lopez H, Landis J, Antonio J. International Society of Sports Nutrition position stand: creatine supplementation and exercise. Journal of the International Society of Sports Nutrition. 2007 Aug 30;4(1):6.
Candow, D. G., Chilibeck, P. D., Gordon, J., Vogt, E., Landeryou, T., Kaviani, M., & Paus-Jensen, L. (2021). Effect of 12 months of creatine supplementation and whole-body resistance training on measures of bone, muscle and strength in older males. Nutrition and Health, 27(2), 151-159.
Candow DG, Chilibeck PD, Forbes SC. Creatine supplementation and aging musculoskeletal health. Endocrine. 2014 Apr 1;45(3):354-61.
Candow DG, Chilibeck PD. Potential of creatine supplementation for improving aging bone health. The journal of nutrition, health & aging. 2010 Feb 1;14(2):149-53.
Candow DG, Zello GA, Ling B, Farthing JP, Chilibeck PD, McLeod K, Harris J, Johnson S. Comparison of creatine supplementation before versus after supervised resistance training in healthy older adults. Research in Sports Medicine. 2014 Jan 2;22(1):61-74.
Chilibeck PD, Candow DG, Gordon JJ, Duff WRD, Mason R, Shaw K, et al. A 2-yr randomized controlled trial on creatine supplementation during exercise for postmenopausal bone health. Med Sci Sports Exerc. 2023;55(10):1750–60.
Chilibeck PD, Candow DG, Landeryou T, Kaviani M, Paus-Jenssen L. Effects of creatine and resistance training on bone health in postmenopausal women. Medicine & Science in Sports & Exercise. 2015 Aug 1;47(8):1587-95.
Chilibeck PD, Kaviani M, Candow D, Zello, G. Effect of creatine supplementation during resistance training on lean tissue mass and muscular strength in older adults: a meta-analysis. Open Access Journal of Sports Medicine 2017 Nov 2; 8: 213-226.
Chilibeck PD, Chrusch MJ, Chad KE, Davison KS, Burke DG. Creatine monohydrate and resistance training increase bone mineral content and density in older men. J Nutr Health Aging. 2005;9(5):352–5.
Chrusch MJ, Chilibeck PD, Chad KE, Davison KS, Burke DG. Creatine supplementation combined with resistance training in older men. Medicine & Science in Sports & Exercise. 2001 Dec 1;33(12):2111-7.
Clarke, H. E., Akhavan, N. S., Behl, T. A., Ormsbee, M. J., & Hickner, R. C. (2025). Effect of Creatine Monohydrate Supplementation on Macro- and Microvascular Endothelial Function in Older Adults: A Pilot Study. Nutrients, 17(1), 58. https://doi.org/10.3390/nu17010058
Close GL, Hamilton DL, Philp A, Burke LM, Morton JP. New strategies in sport nutrition to increase exercise performance. Free Radical Biology and Medicine. 2016 Sep 30;98:144-58.
Cornelissen VA, Defoor JG, Stevens A, Schepers D, Hespel P, Decramer M, Mortelmans L, Dobbels F, Vanhaecke J, Fagard RH, Vanhees L. Effect of creatine supplementation as a potential adjuvant therapy to exercise training in cardiac patients: a randomized controlled trial. Clinical rehabilitation. 2010 Nov;24(11):988-99.
Davies, T. W., Watson, N., Pilkington, J. J., McClelland, T. J., Azzopardi, G., Pearse, R. M., … & Puthucheary, Z. (2024). Creatine supplementation for optimization of physical function in the patient at risk of functional disability: A systematic review and meta‐analysis. Journal of Parenteral and Enteral Nutrition, 48(4), 389-405.
Deane CS, Wilkinson DJ, Phillips BE, Smith K, Etheridge T, Atherton PJ. “Nutraceuticals” in relation to human skeletal muscle and exercise. American Journal of Physiology-Endocrinology and Metabolism. 2017 Apr 1;312(4):E282-99.
Devries MC, Phillips SM. Creatine supplementation during resistance training in older adults-a meta-analysis. Med Sci Sports Exerc. 2014;46(6):1194–203
Diaz KM, Howard VJ, Hutto B, Colabianchi N, Vena JE, Safford MM, Blair SN, Hooker SP. Patterns of sedentary behavior and mortality in US Middle-aged and older adults: a national cohort study. Annals of internal medicine. 2017 Oct 3;167(7):465-75.
Dunlop DD, Song J, Arnston EK, Semanik PA, Lee J, Chang RW, Hootman JM. Sedentary time in US older adults associated with disability in activities of daily living independent of physical activity. Journal of physical activity & health. 2015 Jan;12(1):93.
Eijnde BO, Van Leemputte M, Goris M, Labarque V, Taes Y, Verbessem P, Vanhees L, Ramaekers M, Eynde BV, Van Schuylenbergh R, Dom R. Effects of creatine supplementation and exercise training on fitness in men 55–75 yr old. Journal of Applied Physiology. 2003 Aug 1;95(2):818-28.
Eckert, I., Lima, J., & Dariva, A. A. (2025). Creatine supplementation for treating symptoms of depression: a systematic review and meta-analysis. British Journal of Nutrition, 1-37.
Faager G, Söderlund K, Sköld CM, Rundgren S, Tollbäck A, Jakobsson P. Creatine supplementation and physical training in patients with COPD: a double blind, placebo-controlled study. Int J Chronic Obstr Pulm Dis. 2006;1(4):445–53.
Figueiredo VC, de Salles BF, Trajano GS. Volume for Muscle Hypertrophy and Health Outcomes: The Most Effective Variable in Resistance Training. Sports Medicine. 2017 Oct 11:1-7.
Gordji-Nejad, A., Matusch, A., Kleedörfer, S. et al. Single dose creatine improves cognitive performance and induces changes in cerebral high energy phosphates during sleep deprivation. Sci Rep 14, 4937 (2024). https://doi.org/10.1038/s41598-024-54249-9
Goudarzian M, Rahimi M, Karimi N, Samadi A, Ajudani R, Sahaf R, Ghavi S. Mobility, Balance, and Muscle Strength Adaptations to Short-Term Whole Body Vibration Training Plus Oral Creatine Supplementation in Elderly Women. Asian Journal of Sports Medicine. 2017 Mar 1;8(1).
Gualano B, Macedo AR, Alves CR, Roschel H, Benatti FB, Takayama L, de Sá Pinto AL, Lima FR, Pereira RM. Creatine supplementation and resistance training in vulnerable older women: a randomized double-blind placebo-controlled clinical trial. Experimental gerontology. 2014 May 31;53:7-15.
Gualano B, Rawson ES, Candow DG, Chilibeck PD. Creatine supplementation in the aging population: effects on skeletal muscle, bone and brain. Amino acids. 2016 Aug 1;48(8):1793-805.
Hass CJ, Collins MA, Juncos JL. Resistance training with creatine monohydrate improves upper-body strength in patients with Parkinson disease: A randomized trial. Neurorehabilit Neural Repair. 2007;21(2):107–15.
Hultman E, Soderlund K, Timmons JA, Cederblad G, Greenhaff PL. Muscle creatine loading in men. Journal of applied physiology. 1996 Jul 1;81(1):232-7
Johannsmeyer S, Candow DG, Brahms CM, Michel D, Zello GA. Effect of creatine supplementation and drop-set resistance training in untrained aging adults. Experimental gerontology. 2016 Oct 31;83:112-9.
Kreider RB, Kalman DS, Antonio J, Ziegenfuss TN, Wildman R, Collins R, Candow DG, Kleiner SM, Almada AL, Lopez HL. International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. Journal of the International Society of Sports Nutrition. 2017 Jun 13;14(1):18.
Kuriansky J, Gurland B. The performance test of activities of daily living. The International Journal of Aging & Human Development.1976; 7:343-352.
Kushmerick MJ, Moerland TS, Wiseman RW. Mammalian skeletal muscle fibers distinguished by contents of phosphocreatine, ATP, and Pi. Proceedings of the National Academy of Sciences. 1992 Aug 15;89(16):7521-5
Liu, S., Huang, N., Wu, W., OuYang, X., Luo, Y., Zhong, Y., … & Xiao, L. (2025). The impact of creatine supplementation associated with resistance training on muscular strength and lean tissue mass in the aged: a systematic review and meta-analysis. European Review of Aging and Physical Activity.
Lobo DM, Tritto AC, da Silva LR, de Oliveira PB, Benatti FB, Roschel H, Nieß B, Gualano B, Pereira RM. Effects of long-term low-dose dietary creatine supplementation in older women. Experimental gerontology. 2015 Oct 31;70:97-104.
Neves Jr M, Gualano B, Roschel H, Fuller R, Benatti FB, Pinto AL, Lima FR, Pereira RM, Lancha Jr AH, Bonfa E. Beneficial effect of creatine supplementation in knee osteoarthritis. Medicine and science in sports and exercise. 2011 Aug;43(8):1538-43.
Nilwik R, Snijders T, Leenders M, Groen BB, van Kranenburg J, Verdijk LB, van Loon LJ. The decline in skeletal muscle mass with aging is mainly attributed to a reduction in type II muscle fiber size. Experimental gerontology. 2013 May 31;48(5):492-8.
Oliveira, C. L., Antunes, B. D. M. M., Gomes, A. C., Lira, F. S., Pimentel, G. D., Boulé, N. G., & Mota, J. F. (2020). Creatine supplementation does not promote additional effects on inflammation and insulin resistance in older adults: A pilot randomized, double-blind, placebo-controlled trial. Clinical nutrition ESPEN, 38, 94-98.
Phillips SM. Nutritional supplements in support of resistance exercise to counter age-related sarcopenia. Advances in Nutrition: An International Review Journal. 2015 Jul 1;6(4):452-60.
Pinto CL, Botelho PB, Carneiro JA, Mota JF. Impact of creatine supplementation in combination with resistance training on lean mass in the elderly. Journal of cachexia, sarcopenia and muscle. 2016 Sep 1;7(4):413-21.
Prokopidis K, Giannos P, Triantafyllidis KK, Kechagias KS, Forbes SC, Candow DG. Effects of creatine supplementation on memory in healthy individuals: a systematic review and meta-analysis of randomized controlled trials. Nutr Rev. 2023 Mar 10;81(4):416-427. doi: 10.1093/nutrit/nuac064. PMID: 35984306; PMCID: PMC9999677.
Ralston GW, Kilgore L, Wyatt FB, Baker JS. The Effect of Weekly Set Volume on Strength Gain: A Meta-Analysis. Sports Medicine. 2017 Jul 28:1-7.
Ramos-Hernández, R., Miguel-Ortega, Á., Martínez-Ferrán, M., Fernández-Lázaro, D., Busto, N., & Mielgo-Ayuso, J. (2025). Combined creatine and HMB co-supplementation improves functional strength independent of muscle mass in physically active older adults: a randomized crossover trial. GeroScience, 1-19.
Rhea MR. Determining the magnitude of treatment effects in strength training research through the use of the effect size. Journal of strength and conditioning research. 2004 Nov 1;18:918-20.
Roschel, H., Hayashi, A. P., Fernandes, A. L., Jambassi-Filho, J. C., Hevia-Larraín, V., de Capitani, M., … & Gualano, B. (2021). Supplement-based nutritional strategies to tackle frailty: A multifactorial, double-blind, randomized placebo-controlled trial. Clinical Nutrition, 40(8), 4849-4858.
Schoenfeld BJ, Ogborn D, Krieger JW. Dose-response relationship between weekly resistance training volume and increases in muscle mass: A systematic review and meta-analysis. Journal of sports sciences. 2017a Jun 3;35(11):1073-82.
Schoenfeld BJ, Ogborn D, Krieger JW. The dose–response relationship between resistance training volume and muscle hypertrophy: are there really still any doubts?. Journal of sports sciences. 2017b Oct 18;35(20):1985-7.
Sharifian, G., Aseminia, P., Heidary, D., & Esformes, J. I. (2025). Impact of creatine supplementation and exercise training in older adults: a systematic review and meta-analysis. European Review of Aging and Physical Activity, 22(1), 1-14.
Smolarek et al. (2020). Effect of 16 weeks of strength training and creatine supplementation on strength and cognition in older adults: a pilot study. Journal of Exercise Physiology online, 23(4).
Sullivan, Gail M., and Richard Feinn. “Using effect size—or why the P value is not enough.” Journal of graduate medical education 4, no. 3 2012: 279-282.
Syrotuik DG, Bell GJ. Acute creatine monohydrate supplementation: A descriptive physiological profile of responders vs. nonresponders. The Journal of Strength & Conditioning Research. 2004 Aug 1;18(3):610-7.
Tarnopolsky M, Zimmer A, Paikin J, et al., Creatine monohydrate and conjugated linoleic acid improve strength and body composition following resistance exercise in older adults. PLoS One. 2007;2(10):e991.
Teixeira, L. F. M., Garramona, F. T., & Uchida, M. C. (2024). Impact Of Creatine Monohydrate Supplementation On Balance In Sedentary Non-sarcopenic Elderly Women: 379. Medicine & Science in Sports & Exercise, 56(10S), 128-128.
For local Townsville residents interested in FitGreyStrong’s Exercise Physiology services or exercise programs designed to improve muscular strength, physical function (how you move around during the day) and quality of life or programs to enhance athletic performance, contact FitGreyStrong@outlook.com or phone 0499 846 955 for a confidential discussion.
For other Australian residents or oversees readers interested in our services, please see here.
Disclaimer: All contents of the FitGreyStrong website/blog are provided for information and education purposes only. Those interested in making changes to their exercise, lifestyle, dietary, supplement or medication regimens should consult a relevantly qualified and competent health care professional. Those who decide to apply or implement any of the information, advice, and/or recommendations on this website do so knowingly and at their own risk. The owner and any contributors to this site accept no responsibility or liability whatsoever for any harm caused, real or imagined, from the use or distribution of information found at FitGreyStrong. Please leave this site immediately if you, the reader, find any of these conditions not acceptable.
© FitGreyStrong
- The term resistance training will be used rather than strength training because it captures the full spectrum of goals—strength, muscle mass, power, endurance, joint and bone health, metabolic, cognitive, mental health. It’s a broader, more accurate term that reflects everything older adults can achieve beyond just getting stronger. ↩︎
- For readers of this article, if you think I have missed any studies that should be included, please feel free to contact me via email or leave a comment below. ↩︎
Last updated: January 1st 2026



V well researched and thought through article Sean. I hope you’re well. Darren
Thanks Darren. Glad you liked the article. Hope you’re doing well too. Sean