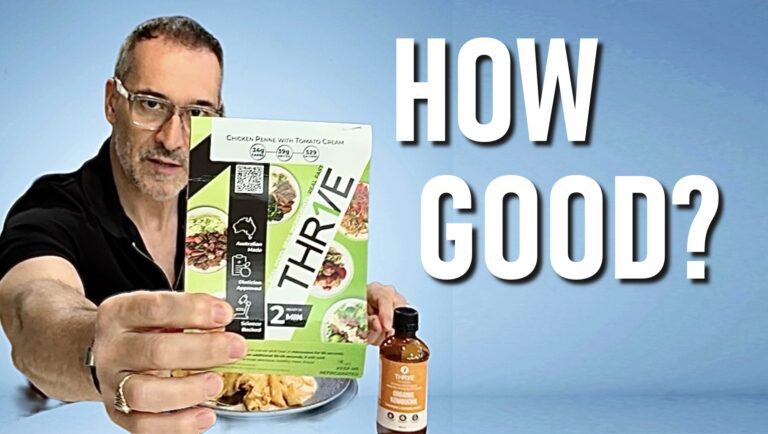
I Tried Thrive Meals — An Honest Review for Adults 50+
Thrive Meals: Review In the video below, I review Thrive Meals (Australia) focusing on convenience, nutrition quality, taste, and practical suitability for adults over 50. I walk through:• Convenience and prep time• Protein content and macro balance• Taste and portion size• How these meals can help make your diet easier• A quick look at the…