Don’t Believe Everything You Watch, Even If It Is A TED Talk!
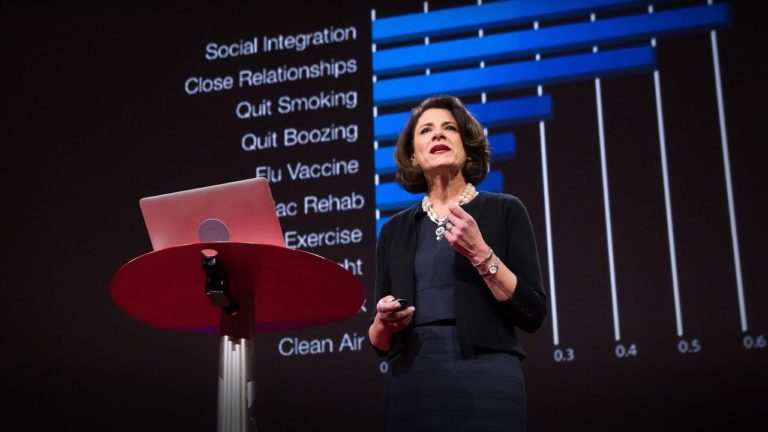
Recently my scientific curiosity was piqued after watching this edited short piece from the TED talk by Susan Pinker. Her presentation titled “The secret to living longer may be your social life” explored (as described in the video) the “least to strongest predictors of reducing your chances of dying”. Now let me be clear. It not my…